The recent U.S. government acknowledgment of UFOs has forced skeptics to confront their past dismissals. Scientist Eric Weinstein apologized for underestimating the UFO community, acknowledging their credibility and urging fellow scientists to investigate UAP seriously. This shift highlights the importance of remaining open-minded to realities beyond perceived boundaries.
Some lines are risky to cross. The line separating fact from fantasy is one such line.
What is remarkable to me about the U.S. government’s recent disclosure of the reality of UFOs, or UAPs, is that even those skeptics who have a reputation for rolling their eyes and bursting forth with ridicule have had to face the truth. Too many people are righteously aware, and claiming they aren’t, doesn’t work anymore. What many smart people have long considered fantasy, is now known to be fact. Confusing fact, perhaps, but fact nevertheless.
This scientist-writer believes that closing your mind to possibilities does nothing more than handicap your consciousness. If you refuse to peer over the boundary of your perceived reality, you’ll limit your awareness. And oh, what interesting things you’ll miss.
Recently I was surprised to read an open apology from a renowned skeptic of the UFO phenomena, a Harvard-trained mathematical physicist and cultural commentator, Eric Weinstein.
Recently, David Bates gave the tweets from Eric Weinstein room on his pages. Not only was Weinstein brutally honest, but I found his challenge to closed-minded scientists especially refreshing.
Weinstein’s Tweets
From Weinstein’s own tweets, Bates quoted the following.
To all the UFO people who were getting it right: I blew it. I thought you were bored, easily convinced, read too much sci-fi as kids, were easily taken in. I thought there was no way this could ambiguously exist in a world flooded with sensors. I thought you were not getting it.
I am very late to your party and even having gotten the report mostly right, it has been exceptionally unpleasant to get in front of it by even a few months. I can only imagine how it feels after the many years the US has gaslight you all while knowing you were not wrong.
A lot of UFO people are nutty. But you the careful community that called balls and strikes as best you could with limited information deserve not only rehabilitation in the minds of the public, but some official recognition that you are to be listened to in the future. Thank you.
I believe you now when you say that there is even much more high quality data available but that it has not been released. At a personal level: You were right, I was wrong. Thanks for letting me join you at the ‘last minute’ in the few months before the report. I’ll listen more.
I also wanted to say to the non-ufo community that whatever I got right largely didn’t come from me. It came from patriots, fellow scientists & others who were not taken in the way I was. All I did was a bit of filtering and after-market analysis given the gravity of the issue.
According to Bates, Weinstein followed up a few hours later.
It’s totally irresponsible for any scientist to refuse to investigate UAP after this report with a full and unpruned decision tree at her side. That includes considering the total incompetence of the defense department, *aliens*, spoofing by enemies and UFO political economy.
And US scientists who refuse to take this seriously as per the above tweet are neglecting and/or turning their back on our national and international security responsibilities given this report. That is my belief. Full stop.
Thank you, David Bates, for making these tweets accessible.
Discover More
Seeking an exhaustively compiled account of a particular class of large UFOs, the Triangles? Look no further than the investigative writings of David Marler. In my opinion, as current UFO investigators go, he is the most careful and detailed of them all.
From the cover of Triangular UFOs: An Estimate of the Situation.
I thought the jig was up when I heard the top U.S. Intelligence Agency was releasing what it knew about UFOs. (See link at the bottom of this post.)
Who would want to read a science fiction novel about UFOs and aliens when the truth is—as they say—stranger than fiction?
What would happen to all those imagined UFOs that slice through water as easily as air? What about spaceships that are massive quantum computers that sense, think and plot the safest course through a universe littered with obstacles both large and small?
What about ships powered by the free energy of the cosmos, steered by the photonic vibrations of colored lights modulating the propulsive energy at the core of the cosmic vacuum?
What would be the fun in imagining aquatic species able to tolerate high pressures but unable to survive the toxic oxygen in our atmosphere? Where would the mystery go once we knew the truth?
What could inspire awe in reading about humans working with strange creatures who teach us to genetically engineer a new breed of humans to survive coming cosmic cataclysms?
What is the use in imagining, once you know the truth?
Departing for Mars. Illustration from Atmosphere, Book 3 of the Jason Parker Trilogy.
Well, as we now know, science fiction writers needn’t worry. Yes, the U.S. military finally admitted that UFOs exist, which is a vast improvement in government transparency. And, let’s admit it, the reality of UFOs has been one of the worst kept secrets of all time. The darn things keep showing up at the strangest times, sometimes far away, but sometimes incredibly close.
The luckiest humans, those who win the UFO reveal lottery with a closeup view of the craft, have their lives changed forever. This I know. And the number of such human observers are legion.
For reasons known only to the government, their admission of UFOs is not accompanied by the sort of detail for which most UFO aficionados were hoping. But frankly, that is likely a deliberate ploy for reasons of national security. I truly believe, and fully support, the continued need for secrecy.
And because of that secrecy, science fiction writers are still free to imagine what they will. After all, fantasy might be the best way to sow awareness of things we cannot imagine, outside of fiction.
But there are some things that science fiction writers like myself find hard to comprehend. The questions I pose here are ones that in my opinion are of much greater importance than the reality of UFOs, or even ETs from distant star systems.
Frequently, nonscientists attempt to explain the weird nature of some UFO sightings by supposing the craft appear from some bubble of an extradimensional universe. The craft and their supposed inhabitants are perhaps not from a portion of our universe far, far away, but rather they are in fact—right here. Right here as in right next door in a higher dimensional universe, or multiverse!
I repeat, I have heard such things from nonscientists. So, what do scientists think?
With few exceptions, they ignore it. Even the multiverse-believing cosmologists don’t yet have the tools to detect unseen universes. Not seeing is not believing, although to be fair, they may spend a lot of time thinking about it.
I would agree that much of the popular writings on the subject of unreachable dimensions are pseudoscience, or less politely, poppycock. Except for the fact that Einstein once said, “It is entirely possible that behind the perception of our senses, worlds are hidden of which we are unaware.”
So, as a scientist and writer, I hold fast to the fact that long after we know that three-dimensional spacecraft and their alien crews exist, we still will not understand higher dimensional universes. Are there hidden worlds there, as wondered by Einstein, populated with sentient beings?
I wish I knew for sure. I would dearly love to possess a higher dimensional container, a sort of a stripped-down, dumb version of Dr. Who’s Tardis. That way I could discard accumulated junk and never see it again. And I’d never get charged disposal fees.
Free energy would be life changing, but free junk disposal would be the icing on the cake.
Top image: A scene from Atmosphere, book 3 of the Jason Parker Trilogy. (Copyright, 2020, 2021)
Here’s the link to the Preliminary Assessment from the Office of the Director of National Intelligence. (For Jason Parker readers, that’s the same office that fictionally hired Laura Smith to be their Subject Matter Expert on ET Affairs.)
Large scale nuclear accidents like those at Chernobyl and Fukushima are environmental disasters which grab the headlines. But lesser accidents do occur, just as in any industrial facility. I was involved in one such incident.
From the mid-sixties to the mid-nineties, Georgia Tech had a research reactor which served a multitude of research purposes. It also gave Nuclear Engineering students a hands-on experience with a working nuclear reactor.
The Frank H. Neely Nuclear Research Center, contained a 5-megawatt heavy-water (D2O) cooled reactor located on the Georgia Tech campus.
The Georgia Tech Nuclear Reactor and Research Center
In the late 60s, I was a graduate student in the Georgia Tech Department of Biology. I was working for a professor who had an interest in manganese and bacteria. One of his projects was using neutron activation of the manganese ions found in Atlanta’s drinking water supply, Lake Lanier. Elevated manganese levels in water is an indicator of pollution.
After driving to Lake Lanier and launching a small boat, another graduate student and I would pump lake water from 100-feet down up into water sampling jugs on the boat. Our most important sampling site was just offshore a water treatment plant, the currently named Shoal Creek Filter Plant. That plant was less than two miles from the Buford Dam, so the water was reliably deep.
Buford Dam at Lake Lanier, https://saportareport.com/metro-atlantas-drought-far-dust-bowl-far-healthy/columnists/david/
One day, the 100-foot-long sampling line disconnected from its reel and disappeared overboard. Without thinking, I dived over the side of the boat with my glasses and billfold, and swam down after the disappearing line. The yellow-green light was getting dimmer every foot I descended.
I was probably twenty feet down when I caught a blurry sight of the barely visible line sinking rapidly through the water.
As I rose back to the boat with the line in my grasp, my crewmate gave me a look of “What the (expletive deleted) just happened?” He had been looking away when I dived overboard, severely rocking the boat. One second, I was there, and the next second I was gone, almost throwing him into the lake in the process.
That was not the last time he would be surprised, as you will read shortly.
Miraculously, I did not lose my glasses, but all my billfold photos were a total loss. But I had saved the research equipment!
Back at the Frank H. Neely Nuclear Research Center, my crewmate and I would send aliquots of the water into the core of the reactor using an air-driven pneumatic system called a “rabbit.” Once in the reactor core, the water sample was bombarded by a dense neutron flux, for a predetermined amount of time.
The floor of the reactor containment building during our time there. The control room is mid-photo.
Georgia Tech reactor control room. We technicians could look but couldn’t touch.
Once the rabbit system pulled the sample out of the core, the sample was measured by Geiger counter to determine if it was safe to approach.
Neutron bombardment produced radioactive isotopes of manganese, converting Mn55 into Mn56. Mn56 has an ideal half-life of 2.6 hours and emits gamma rays at 846.8 keV. Manganese is easy to detect with gamma spectroscopy.
Due to the low level of manganese in the fresh water samples, the Geiger counter never indicated the sample was “hot” after its trip to nuclear hell.
Neutron Activation and radioactive decay. Element X has a mass A and charge Z. Absorption of a neutron increases A by 1. Beta particles can have either a negative charge (like electrons) or a positive charge (positrons) so the result of beta decay can yield a net positive or negative charge. https://nmi3.eu/neutron-research/techniques-for-/chemical-analysis.html
We prepared the lake water samples in a clean room environment. That is also where we returned the newly radioactive sample, transferring it to a sample cell placed in the lead-lined spectrometer. Of course, we always wore full isotope protection (disposable gloves, gowns and masks.)
Modern day laboratory equipment for determination of γ-radiation spectrum with a scintillation counter. The output from the scintillation counter goes to a Multichannel Analyzer which processes and formats the data. By Manticorp – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=17598452
After gamma ray measurements were taken, the radioactive samples were placed in lead-lined cavities for disposal by reactor staff.
Our work progressed without incident until the professor asked us to activate a sample of saltwater. Neutron activation of Cl35, the natural form of chlorine, produces Cl36, with a half-life of 301,000 years.
We noted that as the rabbit returned with its sample of saltwater from its trip into the reactor core, the sample was extremely hot (radioactive), due no doubt to the high concentration of chlorine in salt water. After letting it cool a bit (some chlorine isotopes decay quickly), we performed our usual sample transfer and measurements.
Cl36 is a weak gamma emitter, but we had a hot enough dose to pick it up on the gamma spectrometer. The primary decay mechanism for Cl36 is through low-energy beta particles.
The radiation doses and half-lives had always been low and short for the manganese fresh water samples, and thus we were not in the habit of placing our hands and feet through a radiation detector prior to leaving the reactor research building. That dosimeter was intended for “hot” work.
As usual, it was late in the day when we finished our work, and few people remained in the building. Before exiting the building after our seawater work, we passed by the usually ignored detector.
But that day, I turned around and said, “Let’s check ourselves, just to be sure.”
I was clean, as I had expected. But as my colleague put his hands and feet into the device, screeching alarms and flashing red lights stunned us. As we southerners say, it caused a commotion.
I had heard that nuclear danger alarm only once before, without knowing the cause of it. But now, we were the center of attention. The few people remaining in the building surrounded us within seconds, or so it seemed. Apparently, running towards danger is for all kinds of first responders.
After the staff carefully examined our discarded gloves, masks and garments, they discovered that one of the gloves had a small tear in the right-hand thumb. That small tear was all it took to contaminate my friend.
It was late at night before we were cleared to leave, and then only with extensive washing of my colleague’s right hand. The radiation safety officer wrapped a thick layer of gauze around the offending thumb, and securely taped it. And then he got to work on a lot of paperwork.
Unlike the Mn isotopes we normally worked with, the Cl36 isotope would not decay for many human lifetimes. So, scrubbing and dilution was the only solution.
The thumb was heavily bandaged because the only risk was to the student’s new baby. Beta particles, essentially electrons, cannot penetrate deeply to vital organs, so Cl36 residue was not as much of a concern as would be gamma emitters. However, if the baby had sucked on the father’s thumb, the way teething babies do, the Cl36 isotope would have been ingested. And beta radiation occurring internally can be a health risk.
And to think, we almost let my friend go straight home to take over baby duty.
My fellow student was warned to keep his distance from his baby, and wash his hands thoroughly several times a day, rewrapping his thumb with fresh gauze after every wash. After a week of that repetitive washing routine, it would likely be safe for him to cuddle his baby girl once again, after one last Geiger Counter check.
In the meantime, he was excused from diaper duty!
This type of contamination incident may be more common than you think. Fortunately, it did not equate to a calamity. But it could have been a calamity for that little girl and her family had she ingested radioactive chlorine atoms.
Those dealing with radioactive materials, high pressure, dangerous chemicals, fires, and carrier flight decks, to name just a few hazards, know that personal disaster is only a misstep away. In spite of training, humans do make mistakes. But fortunately, this mistake was caught in the nick of time.
Just like skeletal muscles, respiratory muscles have a limited ability to respond to respiratory loads. An excellent example of this is a person’s inability to breathe through an overly long snorkel (Figure 1.) Our respiratory muscles simply aren’t strong enough to overcome the pressure difference between water depth and the surface.
This doesn’t work. Her respiratory muscles are not strong enough. Illustration by Cameron Cottrill.
The primary respiratory muscle is the diaphragm, (the brown organ lying below the lungs in Figure 2.) The diaphragm is designed for low-intensity work maintained 24/7 for the entirety of your life.
Like the heart muscle, its specialty is endurance. When called upon to maximally perform, the diaphragm needs assistance.
That assistance is provided by the accessory respiratory muscles, primarily the intercostal muscles linking the ribs within the rib cage.
The human diaphragm separating the lungs from the abdominal cavity. Graphic by John Clarke.
Unless you’re reading this while running on a treadmill, your body is probably idling. Your heart is beating rhythmically, your diaphragm is methodically contracting and relaxing. But, if some dire event were to happen, you would be primed for action. If you needed to react to an emergency, your heart and lungs would race at full speed.
The difference between idling and full-speed capability is called physiological reserve, which in turn is divided into its components; cardiac, muscular, and ventilatory reserve. As drivers, pilots, and boat captains will attest, it’s always good to have fuel reserves. Likewise, physiological reserve is good to have in abundance.
The Dive
The following is an imaginary tale of a young, blond-haired hipster drawn to the Red Sea for a deep dive. He chose to dive on the wall at Ras Mohammed on the Eastern Shore of the Sinai, which descends quickly down to a thousand feet and beyond. That was his target—1,000 feet.
The previous year he bought a rebreather so gas usage should not be a problem for his deep dive. He also sprang for the cost of helium-oxygen diluent. Trimix would have been cheaper, but he spared no expense. Nothing but the best. To that end, he used loose-fill, fine grain Sodalime in his CO2 scrubber canister.
These were his thoughts as he descended.
Free-falling at three hundred feet. Never been this deep before. The water’s getting cold, so the warm gas from the canister feels good.
800 feet. Wow, the gas is thicker now.
When he reached the bottom, he realized something wasn’t right. He sucked harder and harder, feeling his full face mask collapsing around his face with each inhalation. He was “sucking rubber,” feeling like he was running out of gas, but his diluent pressure gage still read 1800 psi.
Unconsciously, he compensated for the respiratory load by slowing his breathing—easing his discomfort. Concerned, he briefly switched to open circuit bailout gas, but that didn’t feel any better. In fact, it was worse, so he switched back to the bag.
Surprisingly, he couldn’t get off the bottom. In fact, he was slipping further downslope. He needed to drop weights, but they were integrated. He fumbled with his vest, trying to remember how to release the weights, but he couldn’t work it out.
He found the pony bottle to inflate his integrated BC, but after a second’s spit of air, it stopped filling. He would have to swim off the bottom. As he struggled to swim upwards in the darkness, and without bubbles to guide him, he wasn’t sure which way was up.
His heart was beating at its maximum rate, trying to force blood through his lungs, but he couldn’t force enough gas in and out of his lungs to clear his bloodstream of its increasingly toxic CO2 load. The build-up of CO2 in the arterial blood was clouding his thinking. The CO2 was making him want to breathe harder, but he couldn’t. The feeling of breathlessness—and impending doom—was overwhelming.
————
The accident investigation on the equipment was inconclusive. The dive computer had flooded, but that was irrelevant. Surface pre-dive checks were passed. The rebreather seemed to function normally when tested in a swimming pool. The investigators convinced a Navy laboratory to press the rebreather down to 1,000 feet, but nothing abnormal was found other than a slight elevation of controlled PO2.
The Analysis
An asthma attack can kill by narrowing the airways in the lung, making the person suffering the attack feel like they’re sucking air through a clogged straw.
A healthy diver doesn’t have airways that constrict, but gas density increases with depth, causing the same effect as a narrowed airway. It becomes increasingly difficult to breathe as depth increases. A previous InDepth blogpost on gas density discusses this subject.
Normal human airways compared to airways during an asthma attack. Graphic courtesy of Asthma and Allergy Foundation of America.
If the strength of respiratory muscles is finite, just as it is for all muscles, then any load placed on those muscles will eat away a diver’s “respiratory reserve.” From the diaphragm’s perspective, the total loading it encounters is divided between that internal to the diver and that external to the diver. As gas density increases, internal loading increases. A rebreather is external to the body, so flow resistance through a rebreather adds to the total load placed on the respiratory muscles. If the internal resistance load increases a lot, as it does at great depth, there is very little reserve left for external resistance, like that of a rebreather.
In this fictional tale of a hapless diver, he needlessly added respiratory resistance by using fine-grain Sodalime in his scrubber canister. Compared to large grain Sodalime, such as Sofnolime 408, fine-grain absorbent adds scrubber duration, but it also increases breathing resistance. It thus cut into the diver’s ventilatory reserve.
This fictional diver exceeded his physiological reserves by,
not understanding the effect of dense gas on the “work of breathing,”
not understanding the limitation of his respiratory muscles, and
by not realizing the “best” Sodalime for dive duration was not the best for breathing resistance.
He also didn’t realize that a rebreather scrubber might remove all CO2 from the expired gas passing through it, but it is ventilation (breathing) that eliminates the body’s CO2 from the diver’s bloodstream. Once CO2 intoxication begins, cognitive and muscular ability quickly decline to the point where self-rescue may be impossible.
Lessons from The U.S. Navy
Considering the seriousness of the topic, it is worthwhile to review the following figures prepared for the U.S. Navy.
First, we define peak-to-peak mouth pressure, a measure of the pressure exerted by a working diver breathing through the external resistance of a rebreather. Total respiratory resistance for a diver comes in two parts: internal and external. In the following figures, those resistances in the upper airways are symbolized by a small opening, and in the external breathing apparatus, by a long, narrow opening representing a UBA attached to the diver’s mouth.
High external resistance. In this case, the difference between mouth pressure and ambient water pressure is called ΔP1 Credit with modifcation: “Direct measurement of pressures involved in vocal exercises using semi-occluded vocal tracts”.Low external resistance. The difference between mouth pressure and ambient water pressure is called ΔP2. Credit with modification: “Direct measurement of pressures involved in vocal exercises using semi-occluded vocal tracts”.Mouth pressure waveforms ΔP1 and ΔP2 during breathing with high (P1) and low (P2) external resistance.
This author reviewed over 250 dives by Navy divers at the Naval Medical Research Institute and the Navy Experimental Diving Unit. These were working dives involving strenuous exercise at simulated depths down to 1500 feet seawater, using gas mixtures ranging from air to nitrox and heliox. Gas densities ranged from about 1 gram per liter (g/L) (air at the surface) to over 8 g/L. Each dive was composed of a team of divers, so each plotted data point had more than one man-dive result included. An “eventful” dive was one where a diver stopped work due to loss of consciousness, or respiratory distress (“dyspnea” in medical terminology.) They were marked as red in the following figure. Uneventful dives were marked in black.
Using a statistical technique called maximum likelihood, the data revealed a sloping line marking a boundary between eventful and uneventful dives.
Peak-to-peak mouth pressure and gas density conspire to increase a diver’s risk of an “event” during a dive.
The fact that the zero-incidence line sloped downward illustrates the fact that the higher the gas density, the greater the respiratory load imposed on a diver by both internal and external (UBA) resistance. The higher that load, the lower the diver’s tolerance to high respiratory pressures.
By measuring peak-to-peak mouth pressures, we are witnessing the effect of UBA flow resistance at high workloads. It does not reveal the flow resistance internal to the body. However, when gas density increases, internal resistance must also increase.
The interrupted lines in the figure illustrate lines of estimated equal probability of an event. The higher the peak-to- peak pressure for a given gas density, the higher the probability of an eventful dive.
Figure 7 suggests that at a gas density of over 8 grams per liter, practical work would be impossible. The only way to make it possible would be to reduce gas density by substituting helium for nitrogen, or substituting hydrogen for helium, and then doing as little work as possible to keep ΔP low.
For our fictional 1,000 foot diver, the gas density would have been between 6 and 7 grams per L. Using a rebreather, there would be virtually no physiological reserve at the bottom. Moderate work against the high breathing resistance at depth would be very likely to result in an “eventful” dive.
Image Citation for medical graphics: Robieux C, Galant C, Lagier A, Legou T, Giovanni A. Direct measurement of pressures involved in vocal exercises using semi-occluded vocal tracts. Logoped Phoniatr Vocol. 2015 Oct;40(3):106-12. doi: 10.3109/14015439.2014.902496. Epub 2014 May 21. PMID: 24850270.
John Clarke, also known as John R. Clarke, Ph.D., is a Navy diving researcher in physiology and physical science. Clarke was an early graduate of the Navy’s Scientist in the Sea Program.During his forty-year governmentcareer, he conducted physiological research onnumerous experimental saturation dives. Two dives were to a pressure equivalent to 1500 fsw.
For twenty- eight years he was the Scientific Director of the Navy Experimental Diving Unit.
Clarke has authored a technothriller-science fiction series called the Jason Parker Trilogy. All three volumes, Middle Waters, Triangle, and Atmosphere, feature saturation diving from depths of 100 feet to 2,500 feet. The deepest dives involve hydreliox, a mixture of helium, hydrogen and oxygen. UFOs, aliens, and an uncaring cosmos lay the framework for political and human intrigue both on and off-planet.
Although now retired, Clarke has worked for NEDU as a Scientist Emeritus. He now runs a consulting company, Clarke Life Support Consulting, LLC. He helps various companies, when he isn’t writing about diving, aviation, and space. His websites are www.johnclarkeonline.com and www.jasonparkertrilogy.com. His thriller series is available at Amazon and Barnes & Noble.
Related Blog Posts – Further Reading for Rebreather Divers
In the preceding blog post, I reminded the reader that the Earth’s supply of helium is limited. It is not a renewable resource.
Being a diving professional, I am not concerned about the consequence of a helium shortage on party balloons. But I am thinking about the potential consequences on diving.
So, knowing that hydrogen has both good and bad traits, it would be prudent to begin thinking about whether or not there is a way to safely substitute hydrogen for helium in technical, scientific, commercial and military diving.
Perhaps the word “bad” is too much of an understatement. Perhaps “horrible” would be a better descriptor for something like the Hindenburg disaster.
With that sobering reminder of what can happen, we now cautiously move on to the science.
First, we begin with the explosion hazard of hydrogen in binary mixtures of hydrogen and oxygen.
For diving in the 10 to 20 bar range, 326 to 653 fsw range, the upper explosion limit is 94.2 molar percent. So that means that if a binary gas mixture contains 96% hydrogen and 4% oxygen, it should not explode when ignited.
Those underlined words are important. An explosive mixture of hydrogen and oxygen will not explode without an ignition source. Proof of that is exhibited in many college introductory chemistry lectures, and documented in the following YouTube video.
Arne Zetterström
As a forecast of our potential future, during World War II, Sweden was deprived of a ready source of helium coming from the U.S. and elsewhere. So, the clever and industrious Arne Zetterström conducted a series of experimental deep, hard hat dives from 1943 to 1945 using a mixture of 96% hydrogen and 4% oxygen on dives ranging from 12 to 17 bar.
Once at depth, Zetterström switched from a non-hydrox gas mixture to the “hydrox” gas mixture. His initial test dive was to 111 msw (362 fsw, 12 bar), progressing through six dives to a maximum depth of 160 msw (522 fsw, 17 bar).
That dive series was successful. Unfortunately, on the last dive on 7 August 1945, Zetterström died tragically when his dive tenders mistakenly pulled him directly to the surface from the bottom depth of 522 fsw. He died from fulminant decompression sickness.
From the above table we see that modern measurements confirm that Zetterström chose his gas mixes wisely. At a 96 mol% of hydrogen, he was above the upper explosion limit. If there had been an unexpected ignition event, his breathing gas mixture would not have exploded.
I have confirmed the oxygen partial pressure for Zetterström’s dives using PTC Mathcad Express 3.1 and will share the process.
First, I show pressure conversions familiar to Navy divers and diving scientists, but not known to most others.
For Zetterström’s 111 msw (362 fsw) dive, the partial pressure of oxygen (PO2) would have been 0.478 atm, at the top end of the target range (0.4 to 0.48) for U.S. Navy chamber oxygen atmosphere during saturation diving. A PO2 of 0.48 is believed to be the highest PO2 tolerated for extended periods. Saturation dives sometimes last over a month.
For Zetterström’s 6th and last dive, to 160 msw (522 fsw), the oxygen partial pressure was 0.7 ata, about half of what it normally is in modern electronic rebreathers with fixed PO2.
A far more detailed story of the Zetterström Hydrox dive series can be found in this book.
Arne Zetterström Memorial Dive
In 2012, the Swedish Historical Diving Society and the Royal Institute of Technology (KTH) Diving Club, Stockholm, conducted an Arne Zetterström Memorial dive to a relatively shallow depth of 40 msw or 131 fsw. The original 96% – 4% ratio of hydrogen and oxygen was maintained, resulting in a gas mixture with a PO2 of 0.20 atm.
As reported in the KTH Dive Club’s Dykloggen (dive log) report of July 2012, the team lead was Ola Lindh, Project Leader and Diver. Åke Larsson, another diver, contributed the following information about that dive.
The Hydrox divers used open circuit scuba, with back mounted air, and for decompression, bottles of hydrox and oxygen.
The Swedish divers did not go deeper than 131 feet because they were just above the mud at that depth in a quarry. Plus, they did not yet have details of Zetterström’s decompression plan for deeper diving.
Today, they do possess the wartime hydrogen decompression plan, so deeper hydrogen dives may be forthcoming.
Three gas mixtures – hydrogen, and air (nitrogen and oxygen)
When you mix an inert gas like nitrogen (or perhaps helium?) with hydrogen and oxygen mixtures, that greatly reduces the explosion hazard. But as this video shows, sooner or later the ratios might change enough to become explosive.
Naval Medical Research Institute
I spent 12 years working as a diving biomedical researcher at the Naval Medical Research Institute (NMRI) in Bethesda, MD.
Main entrance to the Albert R. Behnke Diving Medicine Research Center, at NMRI.
My laboratory was in the Behnke Diving Medicine Research Center building, but the hyperbaric hydrogen facility was situated a safe distance behind the main building. In the unlikely event of an explosion, the main Behnke facility and its hyperbaric chamber complex would be preserved.
The hyperbaric hydrogen facility was used to test the effects of high-pressure hydrogen and biochemical decompression on pigs, rather than risk human divers. And all of that was done safely, thanks to the professionalism of Navy divers and scientists.
Dr. Susan Kayar checking on the hydrogen diving pigs.
Kayar, a member of the Women Divers Hall of Fame, used at 230 msw (751 fsw) a gas mixture of 88% hydrogen, 2% oxygen, balance helium with a slight amount of nitrogen. That 88% hydrogen mixture put the gas mixture well above the 71.3% upper explosion limit for three gas components at 24 bar pressure. The resulting PO2 was 0.5 ata.
Compagnie Maritime d’Expertises (COMEX)
COMEX and their human-rated hyperbaric chambers are located in Marseilles, France.
When it came to manned hydrogen diving, the effect of hydrogen narcosis forced COMEX to operate below the upper explosion limit during its long series of experimental hydrogen dives.
In 1985, COMEX’s Hydra V was the first manned hydrogen dive to 450 msw. Hydrogen fraction was 54%, helium fraction was 45%, and oxygen fraction 1%. PO2 was a nominal 0.45 atm, the same partial pressure used by the U.S. Navy for saturation dives.
In 1988 during Hydra VIII, the first open water hydrogen dive, the depth was 534 msw, or 1752 fsw. Hydrogen fraction was 49%, helium fraction was 50%, and oxygen fraction 1%. The resulting oxygen partial pressure was 0.54 atmospheres.
The following video documents the record-breaking Hydra VIII dive.
The 534 msw Hydra VIII depth record was broken by Hydra X, a 701 msw, 2300 fsw chamber dive. The gas mixture was the same as in Hydra VIII, hydrogen fraction 49%, helium 50%, and oxygen percentage 1%. Due to the increase in depth, PO2 rose to 0.7 atm, an oxygen partial pressure frequently used in older U.S. Navy rebreathers.
The head of the Diving Medicine Department at NMRI, CAPT Ed Flynn, M.D. (glasses and grey hair sitting on the right side of the console), was performing physiological studies on both Hydra VI and VIII. In essence he was the Patron Saint of the NMRI Hydrogen Research Facility.
Shallow Hydrogen Diving
What have the previous studies taught us? Well, for one thing, the Swedes showed in their Arne Zetterström Memorial dive that you can get away with oxygen concentrations close to normoxia, PO2~0.21 ata. The disadvantage of normal atmospheric partial pressures of oxygen, compared to higher pressures, is related to decompression time. There is a decompression advantage when breathing oxygen pressures of 1.3 to 1.45 ata. Virtually all modern electronic rebreathers use those oxygen pressures for that reason. But as the KTH Dive Club showed, hydrogen decompression can be safely handled at relatively shallow depths.
For recreational divers, there is an economic advantage for reducing helium usage by substituting nitrogen. We don’t yet know what the economic and safety comparison would be when using helium diluted hydrogen versus pure hydrogen.
Hydrogen, helium, and oxygen were the standard gases used by COMEX. But they were likely chosen to lessen hydrogen toxicity. Hydrogen toxicity would not be a problem at shallow depth. And in fact, the KTH Dive Club reported no toxicity problems.
Retrospection
As proud as I have been of the record-breaking COMEX hydrogen research program, and of the highly imaginative U.S. Navy hydrogen research program, it has not been lost on me that the first deep human hydrogen dives were conducted by an undoubtedly low-cost program led by a single Swedish Naval Officer, Arne Zetterström.
Now, I find it remarkable that the people testing hydrogen diving at relatively shallow depths, would also be Swedish. Unlike the COMEX and NMRI projects described above, I suspect the KTH Dive club was not sponsored by multimillion dollar programs.
You have to admire the Swedish chutzpah.
Disclaimer: The author is no longer employed by the Navy or Department of Defense. All opinions are my own, and not those of any government agency. This document is posted purely for historical and educational interest. At risk of violent death, under no circumstances should the reader be tempted to explore the production, storage, or use of hydrogen without thorough and certified safety training.
Helium is a low density, non-narcotic gas often added to the breathing gas mixture of divers who have to dive deep. Nitrogen, the primary component of air is both dense, making it hard to breathe when diving deep, and narcotic at depths below one hundred feet. That is why nitrogen leads to the so-called “rapture of the deep.” Narcotic divers make bad decisions.
If it weren’t for helium, some of the deepest and most sensitive diving for national security would never have happened. So, it’s really important. Commercial saturation diving in the oil fields of the North Atlantic and the Gulf of Mexico is wholly dependent on the easy to breathe and non-narcotic properties of helium.
Both civilian and government science divers, technical divers, and underwater cave explorers have been able to extend their diving range and safety because of helium in their breathing gas.
Helium graphic from the cover of a 2016 report on helium supply shortages by the American Physical Society, the American Chemical Society, and the Materials Research Society. — Image credit – Ashley Mumford
For those not familiar with the second lightest gas in the periodic table, I’ve included a Fast Fact from the Bureau of Land Management (BLM) at the end of this post.
There are two drawbacks to helium. A source of breathable helium is sometimes hard to locate, and the gas is expensive. Because of that expense and growing scarcity, it is forecast to become increasingly difficult to find, especially in remote locations.
From a Science Direct article, “Ongoing ascent to the helium production plateau – Insights from System Dynamics” in Resources Policy, Vol. 35, Issue 2, June 2010, pgs 77-89.
The primary source of helium, a non-renewable resource, is from gas wells. As shown in the BLM summary at the bottom of this post, the demand for helium is high in scientific, medical, military, and commercial applications.
Cryomodules for an x-ray light source LCLS-II are under construction at Fermilab in Illinois. The cryomodules will house superconducting cavities that are cooled with liquid helium. Credit: Reidar Hahn.
Not on the list, and the least likely to be considered during allocation of an increasingly scarce resource, is civilian diving, and perhaps even military diving.
The above graphical projection made in 2010 does not consider the damping effect of current government policies which make drilling oil and gas wells, and fossil fuels in general, undesirable. While Qatar and Russia have significant helium reserves, helium transported from distant countries will come with a much higher price tag than forecast in 2010. Unfortunately, no one has so far calculated the net cost of reducing the recovery of gas from the ground, and the recovery of the helium contained in that natural gas.
Why might the next century bring a lowering of helium prices as predicted in the graph above? As I’ve explained in Atmosphere, Book 3 of the Jason Parker Trilogy, fusion reactors should hopefully be common place by then, and helium is a byproduct of those fusion reactions. Of course, the above graph reflects a great deal of uncertainty about the next century, even without the uncertainty introduced by government policies. But our immediate concern is this century, not the next.
One approach to helium conservation is by using rebreathers to conserve gas rather than exhaust it into the water column, as is done in open circuit diving like that pictured in the first underwater photo with two Navy divers. In rebreathers, the only helium wasted is that used to keep breathing bags inflated on descent. Unfortunately, that gas is “burped-off” as gas expands on ascent. But the amount of inert gas wasted during rebreather operations is still far less than in open-circuit diving.
A Navy EX-19 rebreather being tested in Morrison Springs, FL. Navy photo by Bernie Campoli.
Another option for holding down helium cost, is to use helium in “Trimix”, a mixture of oxygen, nitrogen and helium. Such mixes become popular for use at depths of 200 feet sea water (fsw) and deeper. It minimizes the cost of helium while simultaneously reducing the effect of nitrogen narcosis.
A common trimix is called 21/35, which has 21 percent oxygen, 35 percent helium and 44 percent nitrogen. Another common mixture is 18/45, with 18 percent oxygen and 45 percent helium. Those helium percentages are considerably reduced from that found in a typical military heliox mixture containing no nitrogen.
But even then, using helium for recreational deep diving may become far too expensive for any but the richest recreational divers. Already, it’s reported that scientific and medical instruments like superconducting magnets and MRI machines have been affected by helium shortages.
When it comes to the DoD prioritization of military saturation diving missions compared to other military options, the availability and cost of helium will inevitability factor into the high-level decision tree.
So, is there an alternative to helium use in diving? Well, yes and no. I’ve written in both this blog and in my novels about the use of hydrogen in diving, as has a biomedical researcher friend of mine, Susan Kayar, Ph.D. in her novel, Operation Second Starfish.
Hydrogen is even lighter than helium, but at great depth it is narcotic. One strange thing about hydrogen narcosis is that at great depth it can result in psychotic manifestations in some individuals. Also, at shallow depth, hydrogen can form an explosive mixture with oxygen, an issue I’ll discuss in my next post. So, it has to be used with great care and attention to details.
Interestingly, the math says that at 200 fsw, the depth where trimix is typically used, hydrogen can be safely substituted for helium. However, only experimentation can prove if that prediction is valid or not. But as helium gets scarcer and more expensive, using hydrogen in place of helium is something worth considering.
[DO NOT CONDUCT YOUR OWN EXPERIMENTS WITH HYDROGEN. THERE IS ALWAYS A CHANCE OF INJURY OR DEATH WITH HYDROGEN. THINK OF THE HINDENBURG!]
Below are links to other hydrogen and forward-looking diving posts in this blog.
Helium is an odorless, colorless, and tasteless gas. Helium, more than 99.9 percent pure, is also used in liquid form at -452 degrees Fahrenheit.
Where does helium come from?
Helium occurs with other gasses in pockets beneath the Earth’s surface. The most economical source of helium is natural gas, all of which contains some helium. Natural gas in the States of Texas, Kansas, Colorado, Utah, and Wyoming is richer in helium than what has been recovered from other States.
How is helium produced?
When a gas pocket containing economically recoverable amounts of helium is found, a well is drilled to release the gas. It travels by pipeline to a processing plant where the helium is separated from the other gasses. One method of separation is a cryogenic process, which uses cold temperature differences to split the components. Another process, membrane filtration, uses molecular size difference to split components.
What is helium used for?
Today, helium plays a prominent role in medical imaging (magnetic resonance imaging), fiber optics/semiconductor manufacturing, laser welding, leak detection, superconductivity development, aerospace, defense, and energy programs.
Is helium renewable (does it naturally replenish itself after humans use it)?
No, helium is a non-renewable resource. That is why the Federal Government stored 44 billion cubic feet of helium in a natural gas reservoir at Cliffside, just outside of Amarillo, Texas. Helium was injected into porous rock 3,000 feet below the Earth’s surface during the 1960s. This rock holds gas like a sponge holds water. Two layers of calcium anhydrite cover the rock, acting as a lid. The sides are surrounded by water.
“The U.S. President was on the phone with the President of China when a video from the International Space Station came in from the NASA feed to the Emergency Operations Center. A huge burnt-orange cloud was covering the entire southern Pacific, extending all the way up to Hawaii and down to New Zealand. This was no ordinary nuclear explosion.”
The recent deadly explosion in Beirut, and the science fiction thriller, Atmosphere, book 3 of the Jason Parker Trilogy, both involve a toxic, brownish-orange gas, nitrogen dioxide. Of course, one involvement is fictional, and the other, sadly, is not.
From the first chapter of Atmosphere, we find a description of the effects of a gamma ray burst hitting the Earth. “Rampaging winds began spreading toxic nitrogen dioxide clouds around the planet, and within days, the earth was fully affected.”
Considering the violence with which nitrogen dioxide is associated, the way it is created is relatively simple. Some chemists will no doubt claim that the following discussion is too simplistic, but I’ll let them fill in the blanks, if they so choose. As advertised, this is just the basics.
Given enough energy, and localized temperatures on the order of 3000°C, nitrogen molecules (two atoms of nitrogen, N2) combine with oxygen molecules (two atoms of oxygen, O2) to form a chemically unstable gas, nitric oxide, NO.
In chemical terms, N2 + O2 → 2NO
If the searing NO gas is cooled rapidly in the presence of oxygen molecules, the toxic, brownish-orange gas, nitrogen dioxide, is formed.
It’s been known since at least 1911 that the temperature of an electrical arc (6000° – 8000°C) is enough to cause N2 and O2 to form NO. If the hot gaseous NO is then rapidly cooled, NO2 results.
In the science fiction novel, NO2 was created high in the atmosphere by a cosmic burst of high energy gamma rays (GRB) colliding with nitrogen molecules in the presence of oxygen. Lightning also creates nitrogen dioxide, although in relatively small quantities. But if you increase the energy and the quantity of nitrogen and oxygen, “a huge burnt-orange cloud” would be formed.
Apparently, an industrial fire caused the thermal decomposition of large quantities of ammonium nitrate, which energetically broke down to form massive quantities of nitrogen gas, oxygen and water.
2NH4NO3 → 2N2 + 4H2O + O2.
The resulting high temperature N2 and O2 instantly combined to form the toxic burnt orange cloud of nitrogen dioxide, as seen in the above photo.
The exact mechanism of NO2 formation likely differs among the progenitor sources (GRB, lightning, explosion), but the basics should be the same.
What happened to the poisonous cloud of NO2 after it formed? Unlike what would happen in the upper atmosphere during a GRB, near the surface there is enough moisture for the NO2 to quickly combine with water to form nitric acid.
3 NO2 + H2O → 2 HNO3 + NO
Nitric acid rain would not be pleasant, but would not be as bad as nitrogen dioxide.
So, imagine if you will, a cosmic event (a GRB) far more violent than any man-made explosion. Imagine the entire atmosphere turning into a cloud like that in the photo above. Arguably, that is what would happen after a devastating GRB from within our galaxy.
Actually, that toxic nitrogen dioxide cloud would be the least of the planet’s troubles. It would be a very bad day on Earth.
The good news is that such an event would be very unlikely.
It was dark, the only light coming from the red glowing numerals of my digital alarm clock. I hadn’t set it to alarm—I needed to sleep as long as I could.
It was also quiet in my bedroom, quiet enough for me to hear my breathing as I lay still, trying to sleep. The breath sounds were rhythmic and calming, breathing in with a hiss, and out with a coarser and louder “huh,” endlessly repeated.
I had just been released from our local hospital after five days on oxygen, diagnosed with “respiratory failure” of unknown origin. The medical term for unknown origin is “idiopathic,” but that word added no clarity to what had happened.
What had happened has been described in a previous blog post, a post that correctly warned that if the illness that almost killed me was any indication, we should NOT expect COVID-19 to abate during the hot and humid months in the American South.
Whatever virus I picked up in Thailand in July, seemed to have a predilection for the hot and humid summer weather of Florida. In other words, it had made itself right at home in my lungs. The result was a puzzling but treacherous case of silent hypoxia, or as some have called it, happy hypoxia. In that regard, my respiratory failure was every bit as inexplicable and potentially deadly as COVID-19.
Thankfully, my viral infection had not yet reached the level of transmissibility of COVID-19. Otherwise, my wife of fifty years would certainly have been affected as she sat by my side for those long and frustrating days in the hospital.
But now, it was time for celebration. By sheer willpower and some tricks of the respiratory physiology trade, I had gotten myself discharged from the hospital. But that’s another story.
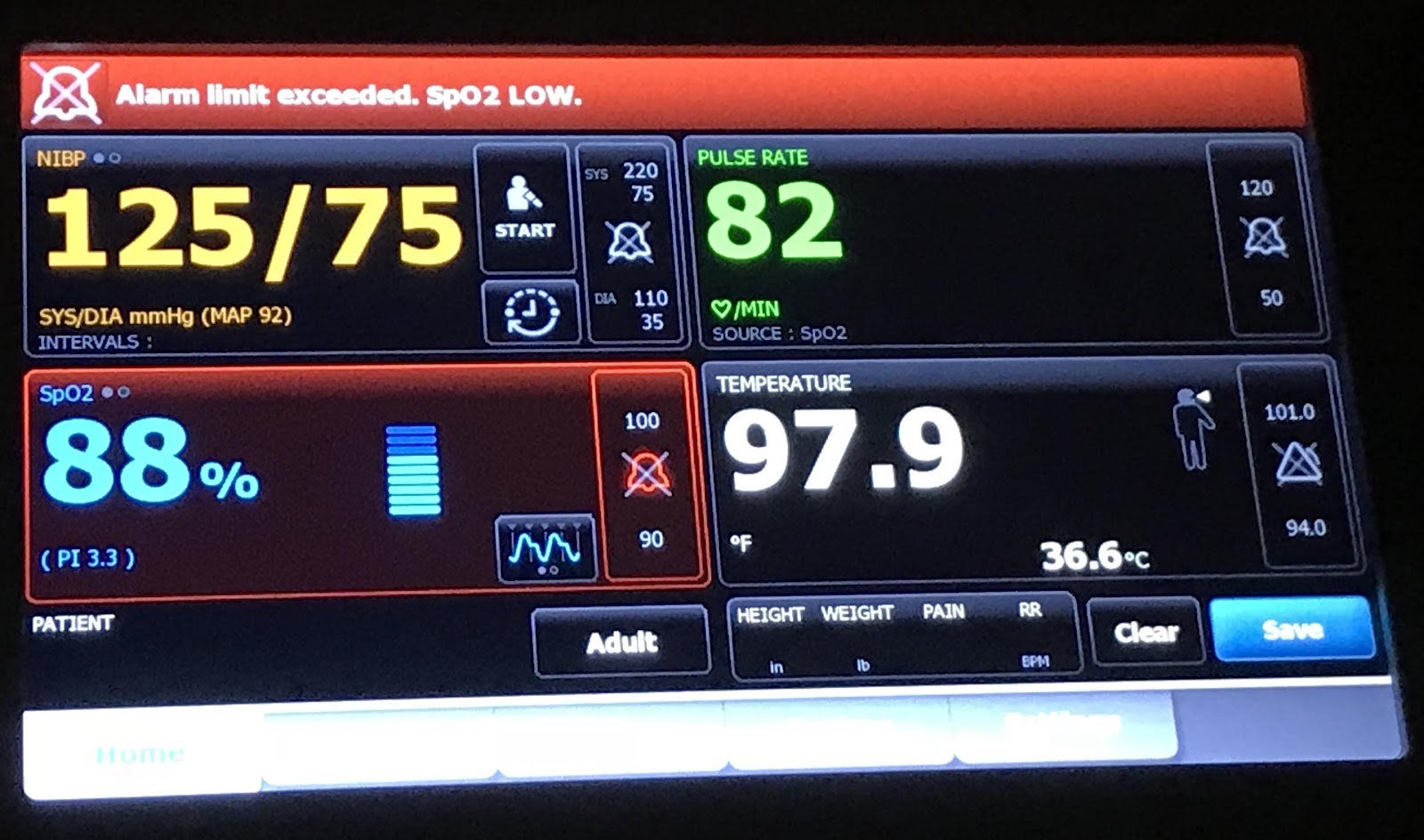
At home once again, my finger-tip pulse oximeter showed I was oxygenating reasonably well on air (in the low 90 percentile), but I was not back to normal (the high 90s). My lungs still had some healing to do before I could claim I was 100% normal.
As I now lay quietly as night enveloped me, entering almost a meditative state listening to my breathing, I noticed a strange sound. Alerted, I listened more intently. And what I heard scared the hell out of me.
There was something alien in my body. I couldn’t feel it, but I could hear it. When I breathed in, it breathed out. When I breathed out, it breathed in. It was clear as day, something was breathing in my chest, and it wasn’t me.
I had a monster in my chest.
At times like that, it is hard to be objective. But with years of training as a scientist, I forced myself to collect data and analyze the results before, well, FREAKING OUT!
The first thing I noticed, was that the asynchrony between my breathing and the other’s breathing, was invariant. They were 180 degrees out of phase, and that never changed.
Professionally, I’ve dealt with probability my entire scientific career. So, if there were in fact some other living thing in my chest, the odds that it would never change its breathing rhythm seemed unlikely. Unless—it was waiting for my lungs to have a full “tidal” breath” before IT took a breath.
Of course! That is exactly what I would do if I was in some giant’s chest. I’d wait until their lungs were full before I’d steal air from them. After all, how else could I, as a little monster, breathe?
But wouldn’t X-rays at the hospital have shown its presence? Well, yes, and no. They didn’t do an MRI. If IT was soft bodied, and growing, it might not have been detected. And going an analytical step further, that could explain why my arterial oxygen saturation levels were not back to normal. IT was stealing oxygen from me.
My heart rate was increasing, which was the last thing I wanted it to do. The more blood I sent the thing, the faster IT would grow. I had to stay calm. But how?
I began thinking about physiology text books. That would put anybody to sleep. But that was also the magic moment. That was when I put a name on the creature in my chest.
I called it, Pendelluft.
Until that night, Pendelluft had been to me of little more than academic interest. I’d read about it, but I knew it is primarily found in patients with chronic obstructive pulmonary disease (COPD); which I do not have. I’ve also never been a smoker or asthmatic.
I knew of the diagrams which explain it, but I never thought that I would be able to hear it, in my body, and especially without a stethoscope.
An illustration of the mechanism of Pendelluft from a humorously named web site, Deranged Physiology.
After I explored the medical literature, I’m not sure anyone in the medical field thinks it possible for a patient to hear his own Pendelluft. But it must be true, since the monster never reared its ugly head, and my arterial oxygen level regained its expected normal value only after the “monster” faded away.
I was pleased when I read that one of my mentors, Dr. Arthur Otis, the one time Department Head of the Physiology Department at the University of Florida School of Medicine, had done the pioneering research on the subject.
However, I found no reference to breath sounds until I came across the 2012 article in the journal Pulmonary Medicine. That study used very complex instrumentation and statistical methodology to detect Pendelluft.
I have to admit that I smiled when I read that 2012 article. I was questioning how much money was spent on that very elaborate medical investigation. Arguably, it was fine work and contributed nicely to the field.
But, I wondered, did they try asking the patient, “Do you hear a monster in your chest?”
The voice on the other end was from the Pentagon. That was the last thing I’d expected to hear on Saturday morning, March 21st, 2020.
On October 1, 2018, I had happily retired after forty years of Federal service. I had remained engaged with the Naval Sea Systems Command and the Navy Experimental Diving Unit as their one and only Volunteer Scientist Emeritus, until I received that call.
Within 90 minutes, I had been reinstated with full security clearance and told to pack my bags.
The next day as I was flying on government orders in an almost empty plane to New Hampshire, I had no idea that the company I was sent to help would begin a ventilator design effort from scratch, that same day. I also couldn’t imagine that the resulting ventilator would receive FDA approval 41 days later.
Wilcox Industries Hybrid Patriot 5510 Life Support System.
The company, Wilcox Industries, in Newington, New Hampshire, has for twenty years built hybrid self-contained breathing apparatus (SCBA) for the military. In fact, twenty years ago, with full Navy support, I helped them design and test their first Scout (now Patriot), life-support system for Tier One operators. But when the COVID Task Force phoned me, Wilcox had no experience with medical devices, especially ventilators. But with the can-do attitude so typical of military support manufacturers, they were willing to learn. In fact, no one I met at Wilcox questioned that it could be done.
Jim Teetzel (center) and Gary Lemire showing me the latest Hybrid Patriot 5510 Life Support System.
All it took was the drive and leadership of Jim W. Teetzel (center of the photo), a brilliant engineer, businessman and CEO who holds more patents than he can probably remember, young engineers who never considered failure being a possibility, a nimble supply system that provided needed parts within 24 hours, and the magic words which opened every door. Those words were, “COVID Task Force.”
Through the Wilcox network of friends and family, patient ventilation circuit parts almost magically appeared, as did the world’s best mechanical Test Lung.
Michigan Instruments Training Test Lung (TTL)
There was nothing I asked for that did not appear almost as soon as I requested it.
Most important for me was the opportunity to teach by showing, by taking pieces of patient tubing circuits and arranging them in a way that would work with a totally new ventilator concept, the Patriot SAVR (Synchronous Automatic Ventilating Resuscitator.)
The Mechanical Engineer, Nick Mercurio, who I call “The Magician,” is working his engineering magic.
Our tasking from the COVID Task Force was not to produce multiple copies of existing sophisticated ventilators that cost as much as a nice car, but to have all hands engaged in producing small, cheap ventilators built to exacting engineering and medical standards. The proof that Wilcox accomplished that goal was the hard won stamp of approval from the Federal Drug Administration (FDA.)
The Software Engineer, Jansen Habrial, or the “Wizard,” makes the SAVR do things I never could have imagined.
While we want Americans to have the finest medical care money can buy, to include BMW-priced ventilators if the need arises, the fact is that during a world pandemic there simply are not enough of those deluxe models to go around. In the most populous nations of the world where per capita income is low, the availability of hundreds of such ventilators are a luxury few if any outlying hospitals can afford. However, low-cost ventilators like the Patriot SAVR fill that need.
Colonel Dodge (ret) and I as I’m departing Wilcox Industries.
Wilcox is blessed with a retired Marine Corp Colonel, Kevin Dodge (on the left side of this photo), Jim Teetzel’s Chief Strategy Officer. Dodge not only has the experience of managing production and testing programs as complex as that for the V-22 Osprey, but has an understanding of the need for strategically placed world markets.
Together, Jim Teetzel, Kevin Dodge, the “wicked” smart Executive Director of International Programs and Lebanese-born Roula Assadi, and Jim’s senior engineers (Nic Goupil, Gary Lemire, Stan Carter) and their Maestro of Quality Assurance, Lorena Grol, have succeeded in turning a small but wealthy Arab nation into a manufacturing center for the Middle East and North African Region, as well as the huge Indo-Asian continent.
A photo of the first Patriot SAVR Q made overseas by the Barzan Industrial Group in Doha, Qatar. It is being held by John Bousquet, one of the young designers from Wilcox Industries.
Considering the tactical pedigree of this ventilator, and the company which built it, I foresee that eventually every U.S. military medic or independent duty corpsman will have one or more of the Patriot SAVR units available at their aid station, just in case any Patriots need saving.
“Happy hypoxia,” or more properly, silent hypoxia, has been one of the most puzzling signs and symptoms of patients presenting to Emergency Rooms with COVID-19. The patient’s arterial oxygen saturation can be in the fifties instead of the normal values in the upper 90s, and yet the patient can be cheerful, fully coherent, and even chatty. Normally, with that low an oxygen concentration in the blood stream, a patient would be in severe respiratory distress.
I experienced silent hypoxia after a visit to Thailand in July of 2018, which makes me wonder: was there a coronavirus lurking in Southeast Asia in 2018 that later mutated to become the killer SARS CoV-2? Did I have SARS CoV-1.5?
Summertime was everything you would expect in Thailand. It was warm and humid, but not uncomfortably so. I had twelve hours ahead of me in the Bangkok Airport waiting for my return flight to Taiwan, then the long leg across the Pacific to Los Angeles. Eventually, I would make my way back to my home in Panama City, Florida, which would also be hot and muggy. No surprises there.
What was a surprise, was that a young lady wandering the airport asked if she could interview me for the Thai Ministry of Tourism. She had official looking IDs, and a load of interview questions. I wasn’t interested, and I was busy, I offered, already tired before the twelve hours of dead time even began.
In truth, I wasn’t that busy, but felt it best not to mingle. I seemed to be the only person not speaking Thai, except for that young lady. Surprisingly, she had no detectable accent and could pass for a Southern California blond.
After a couple of hours, she returned when I could no longer claim to be busy. She had a simple, youthful attractiveness and an unassuming manner. So, tiring of the boredom of waiting, I allowed her to sit beside me while she started running down her list of tourism related questions.
She wanted to know why I came to Thailand. It was to give a talk at a medical and scientific conference on sports medicine. My subject was “Oxygen,” a fact that would soon become ironic. I discovered later that my travel, ostensibly paid for by the Thai Sports Authority, was bankrolled by Beijing. But I didn’t know that at the time.
For 45 minutes the questions continued. They were business-like, the type of questions I would expect from a Tourist Bureau. But one thing caused me concern, her occasional hacky cough. She insisted it was nothing, and I was not alarmed. I thought no more about it as I finally boarded the plane for the first leg of my long journey home.
Eight hours after my arrival in Panama City, I felt ill as I lay in bed, trying to sleep after being exactly twelve hours time-shifted. I felt sicker by the minute. Jet lag doesn’t do that.
By morning, I had suffered chills and sweats, and my physician son insisted I be taken to the closest Emergency Room. As we neared the ER I felt I was going to vomit, and I leaned into a trash can that my wife brought for that purpose.
The next thing I heard was her screaming at me.
I yelled back, completely confused and annoyed. “Why are you yelling at me?”
“I thought you’d died,” she said. “You sighed, threw your back into the seat, and your arms were stiff and shaking.”
Apparently I had passed out from a drop in blood pressure. (I had not yet thought about hypoxemia.)
As I was being monitored in the ER, I felt OK. I conversed with my wife, and was half-joking and half-irritated at my unexpected welcome home event.
After awhile, I began to pay attention to the finger tip pulse-oximeter that was monitoring my arterial oxygen saturation. The reading was slipping lower than I had ever seen before, but neither the nursing staff nor the attending physician seemed the least bit concerned. My wife and I continued to chat. I was not in any discomfort, and ignored the monitors until I caught sight of the updated pulse-ox reading. It had plummeted down to a horrifically low 55%.
I told my wife to alert the nurse. They finally started me on a nasal cannula with oxygen. (For those who know, that was an incredibly delayed reaction.) I also knew enough to realize I should be almost stuporous, yet I wasn’t. I was content, except for my circumstances.
Within a few minutes, an ambulance transported me to a real hospital. Being aware of my overseas travel, they assumed I had a pulmonary embolism, which if detected, would have required immediate surgery. But after a perfusion scan, nothing abnormal was revealed.
After settling into a room, I had zero desire for any of the food they brought me. It was all tasteless, and remained that way for two days.
Initially they kept me on 3 liters of oxygen per minute by nasal cannula, which still wasn’t bringing my oxygen saturation above 84 percent. That was a problem.
At the urging of the CDC, the nursing staff came to my room fully gowned and face-shielded, and stuck that infamously long sampling swab up my nose. They tested me for the most recent viral illness in Southeast Asia at the time, the H7N9 Bird Flu virus of 2017. The results were negative.
In spite of my growing displeasure with being in the hospital, and not tolerating the taste, or lack thereof, of their food, I was happy and chatty with the nursing staff. But neither I, a respiratory physiologist, nor the medical staff could figure out what was wrong. My X-rays showed some consolidation in my lingula, a small lobe in the middle of my lungs, but that was not enough to cause hypoxia of the level I was experiencing.
After a while, I began to get a few signs of pneumonia in my lower lung lobes, but not enough to cause any discomfort, or difficulty breathing. While physicians clobbered the growing infection with antibiotics and steroids, I remained happily hypoxic.
After five days in the hospital, and slowly watching my oxygen saturation rise, a respiratory therapist snuck behind me and turned off the oxygen. My saturation remained low, at 88%, but it didn’t drop further.
That meant, I would remain on air until discharge. That encouraged me enough to call for a walking test, walking down the hospital corridor breathing nothing but air. Unfortunately, I failed that test, and was sent back to bed.
About that time, a pulmonologist came by and told me I had a good bit of atelectasis (collapsed alveoli or lung sacs) in my lower lobes. Finally, something I could fix. I knew what to do.
I wore out my incentive spirometer over the next couple of hours, and then called for another walking test. The Respiratory Therapist chided me…I would just fail again, she said. But I do love a challenge. With her by my side, I moved slowly down the hall, refusing to talk, and that time my oxygen saturation did not drop.
Due to that walking test, I was discharged from the hospital with an oxygen saturation of 92% and returned home to fully recover. (That is in itself an interesting story which I’ll write about next.)
However, the point of this post is that as I read about COVID-19, I’m finding that physicians are puzzled about some of the same bizarre symptoms I experienced in 2018, notably a silent hypoxia. I was never “short of breath” as would be expected with an arterial saturation in the fifties.
From my studies of respiratory physiology, I knew that what had happened to me in 2018 should not have happened, according to the text books. I did not have the SARS virus identified in 2017. But viruses mutate constantly. Could my symptoms have been the signs of a predecessor or cousin to COVID-19? Could it have been an unrecognized COVID-18?
When lungs are not filled with fluid from rampant pneumonia, the most likely way to become hypoxic breathing air is through something called ventilation-perfusion (V-Q) mismatch. A pulmonary embolus can cause massive V-Q mismatch, and can quickly kill if untreated.
However, a recent Science article suggested that COVID-19 might cause microemboli resulting in silent hypoxia. It seems reasonable that enough microemboli, if that’s what it was, could have caused my symptoms in the summer of 2018 without being detected on a pulmonary perfusion scan.
And that worries me for the current pandemic. Summer heat and humidity might not kill this virus. It certainly didn’t kill the virus that I presumably caught from a pretty young girl with a “nothing” of a cough in late July of 2018. It may have been nothing for her, but it was sure something for me.
None of my friends at the medical conference got sick upon returning home. I was the only one spending 45 minutes less than a foot away from that coughing girl. I feel pretty confident where I got it. My only question is, did I pick up a version of coronavirus that was beginning to mutate towards the destructive potential of SARS CoV-2 which erupted just over a year later?
As for the statue at the beginning of this blog post? It is the Yaksha Guardian Giant at the Bangkok Suvarnabhumi airport. If you ask me, he failed completely at protecting me from a tiny little virus. The guardian was awfully big, but sometimes size does not matter.